
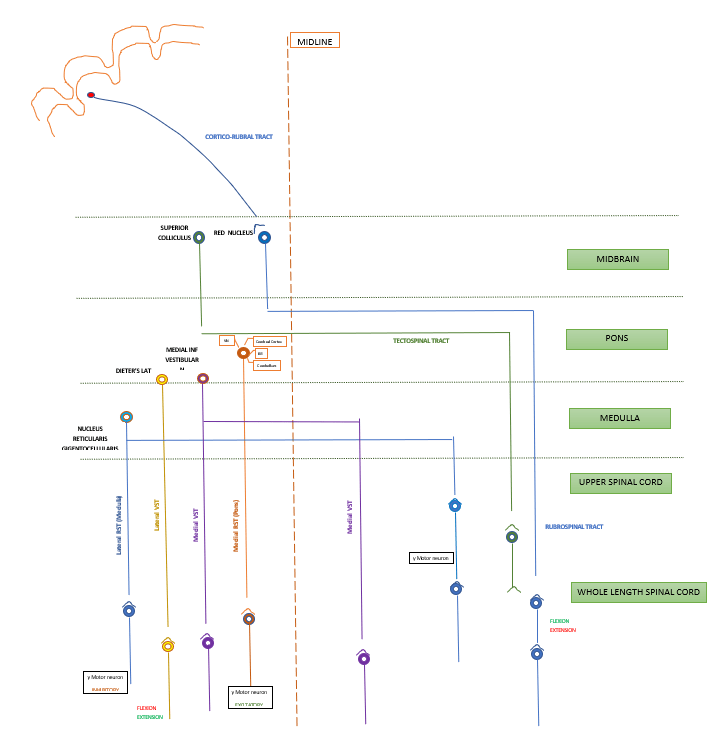
Connect the neurons in,
cerebral cortex , Midbrain, Pons, Medulla & Cerebellum
with
motor neurons (LMN) at various levels.
Axons of UMN synapse on spinal : Alpha motor neuron,gamma motor neuron, Spinal interneuron, Sensory afferents
TRADITIONALLY TRACTS ARE CLASSIFIED AS:

RECENT CLASSIFICATION : Hans Kupyres – 1981,85.

CORTICOSPINAL TRACT / PYRAMIDAL TRACT
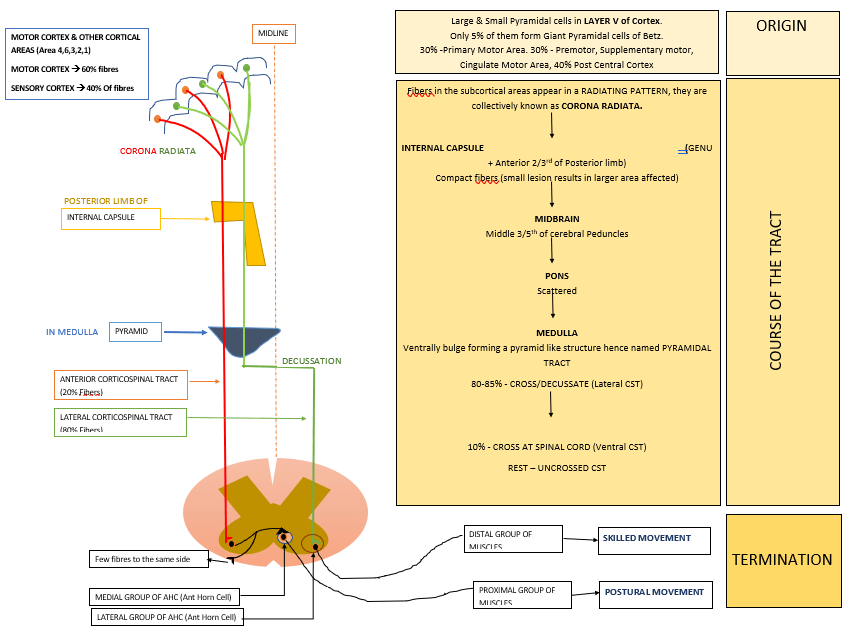
Most important and largest descending tract.
Axons of Cortical neurons descend, form Pyramids in Medulla –> to Spinal Cord (Corticospinal tract)
Some terminate in :
- Brain Stem Reticular formation
- Cranial N Nuclei (V, VII,XII, Corticobulbar Tract) except those supplying to External eye muscle
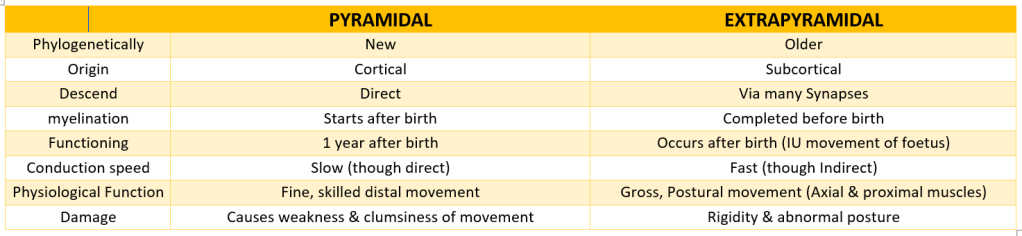
Phylogenetically newest, only in mammals. (No of fibers have progressively increased from monkeys –> Apes –> Man.
1 million fibers (approx.) in human, >90% – small diameter & unmyelinated (SLOW CONDUCTING PATHWAY)
Myelination starts in neonate on 10th – 14th day and completes in 2 years.
NEUROTRANSMITTERS : GLUTAMATE, ASPARTATE.
FUNCTION
- Fine, skillful voluntary movement of Distal limb parts (LCST)
- Postural stability of Axial & proximal muscle.
- influence on stress reflexes.
- Facilitatory (++) –> alpha & gamma where it ends directly. Inhibitory (–) –> via Interneurons
- Efferent limb of superficial reflexes (e.g, abdominal, plantar etc)
- Opposite side lower part of face and hypoglossal (Corticobulbar tract)
- useful in sensori-motor coordination.
- Path of transcortical load compensation mechanism (Increased load –> Increased muscle contraction mediated by Cortex)
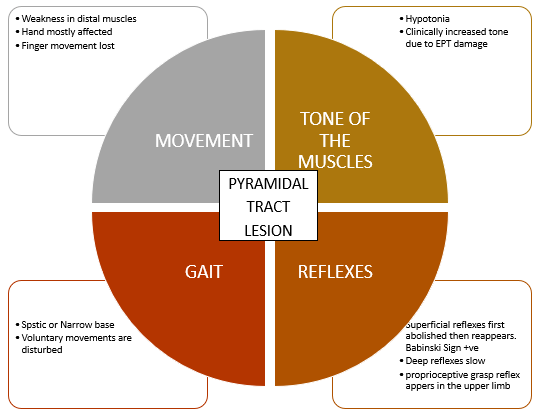
LESION
MOTOR DEFICITS OCCUR DUE TO DESCENDING TRACTS. PURE Pyramidal tract lesions are rare.
ACUTE Lesion (Stage of shock)–> Paralysis of opposite half, No reflexes, Emotions are intact. Lasts for 2-3 weeks. (Symptoms include lesions of both PT+ EPT )
CHRONIC Lesion (Stage of recovery) :
EXTRAPYRAMIDAL TRACT
- Outside Pyramidal tract
- Multineuronal motor system with number of synapses involving many regions of brain.
- All from cortex & subcortical (brainstem) areas other than those in Pyramidal tract.
FUNCTIONS OF EXTRAPYRAMIDAL TRACT
- Regulation of Posture, Equillibrium, Muscle tone
- Coordinated, synchronized movement of head, eye, neck etc
- Provide platform for Pyramidal system to operate fine, skilled movement.
LESIONS IN EXTRAPYRAMIDAL TRACTS:
- MUSCLE TONE – Increased (upper limb – Flexion, Lower limb – Extension)
- ABNORMAL POSTURE
- INVOLUNTARY MOVEMENT – tremor
- LOSS OF RIGHTING/POSTURAL REFLEXES
- DEEP REFLEXES – exaggerated, clonus may appear
- CLASP KNIFE RIGIDITY (Lengthening reaction) present
- PLANTAR REFLEX – Normal/extensor.
