
Hypoxia is O2 deficiency at the tissue level. Traditionally, hypoxia has been divided into four types.
Numerous other classifications have been used, but the four type system is the one which is most widely used and excepted:

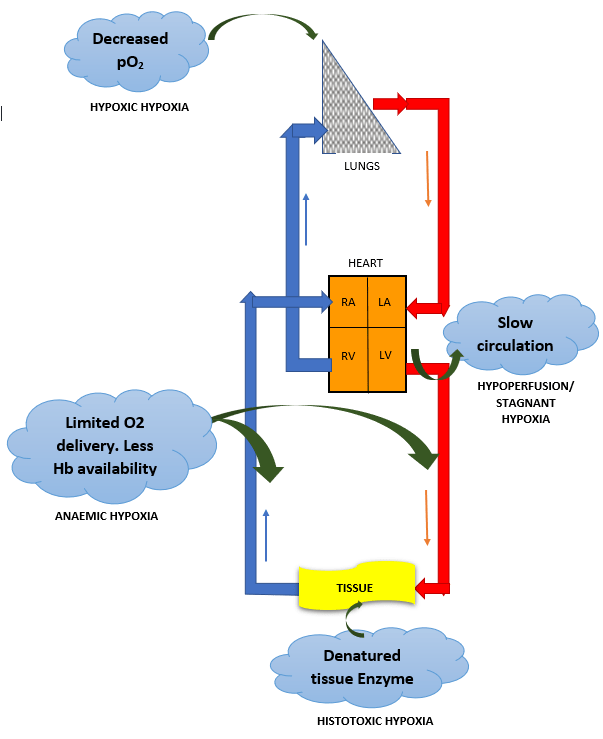
HYPOXIC HYPOXIA
Most common type. A problem seen in NORMAL individuals at HIGH ALTITUDE, complication of PNEUMONIA and many RESPIRATORY COMPLICATIONS. It is a is a condition of reduced arterial pO2
Low arterial pO2
Arterio-venous pO2 difference – LOW
Ventilation – perfusion Imbalance
Venous to arterial Shunt
TREATMENT -Treat the cause. OXYGEN THERAPY

ANAEMIC HYPOXIA
limited ability to deliver O2 to the active tissues. In anemia hypoxia is seen during exercise. Carbon monoxide poisoning – carboxyhemoglobin/COHb, is formed which shifts available HbO2 curve to left and CO has 210 times affinity to Hb than O2 which makes release of CO very slow.
Arterial pO2 normal
Arterio-venous pO2 difference – NORMAL
TREATMENT – Hyperbaric OXYGEN therapy
STAGNANT HYPOXIA
Due to slow circulation and is a problem in organs such as the kidneys and heart OR during shock. The liver and possibly the brain are damaged by hypo perfusion during CONGESTIVE HEART FAILURE.
↑ pCO2 at tissue.
Arterio-venous pO2 difference – INCREASED
TREATMENT – Treat the underlying cause.
HISTOTOXIC HYPOXIA
Due to inhibition of tissue oxidative processes. CAUSE – cyanide poisoning. Cyanide inhibits cytochrome oxidase and possibly other enzymes at TISSUE level. O2 utilization is inhibited.
Tissue cant utilize pO2
Arterio-venous pO2 difference – ABSENT/ALMOST NIL
TREATMENT – Methylene blue or nitrites are used to treat cyanide poisoning. They act by forming methemoglobin, which then reacts with cyanide to form cyanmethemoglobin, a nontoxic compound.
HYPERBARIC Oxygen
Administration of oxygen-rich gas mixtures is of very limited value in hypoperfusion/Stagnant, anemic, and histotoxic hypoxia. Hyperbaric Oxygen helps by increasing the fraction of DISSOLVED Oxygen. Except SHUNT, in other forms of hypoxic hypoxia, O2 is of great benefit.
EFFECT OF HYPOXIA

HAPPY HYPOXIA/HYPOXAEMIA IN COVID-19
COVID -19 infection can bring down the Oxygen saturation, as low as 40 %.
Hypoxia is a warning signal for imminent failure of vital body organs like the kidneys, brain, heart and is usually accompanied by prominent breathlessness. Many patients with pronounced arterial hypoxemia don’t even experience a sense of dyspnea. As a result, in the initial stages of sickness, the COVID-19 patient, on the outside, appears to be alright and “happy” due to lack of any external signals.
The trick to life is to just keep breathing. – Johnny Lung