

PRIMARY MOTOR CORTEX
- Largest of all motor areas
- Lies in the precentral Gyrus –> Area 4 of Brodmann extending from medial surface to lateral sulcus.
- low electrical –> Specific & repeatable movement.
- HOMONCULUS (little man) –> Drawn by Penfield & Rasmussen 1950.
- Body is upside down
- legs most medially
- pharynx lateral most.
- SIZE OF REPRESENTATION – More for body parts for fine & skilled movement (Thumb, Fingers, Face, Pharynx, Vocal cords etc), Less for trunk muscles.
- Lacks LAYER 4 (Granules). So, called AGRANULAR CORTEX.
- Cells are arranged in Columns –> cells from several columns project to same muscles.
- about 30% of Corticospinal Tract fibers take origin
- provide most refined degree of motor control
- Areas enlarge with practice & learning —- CORTICAL PLASTICITY
- LESION — Paresis/paralysis of opposite side
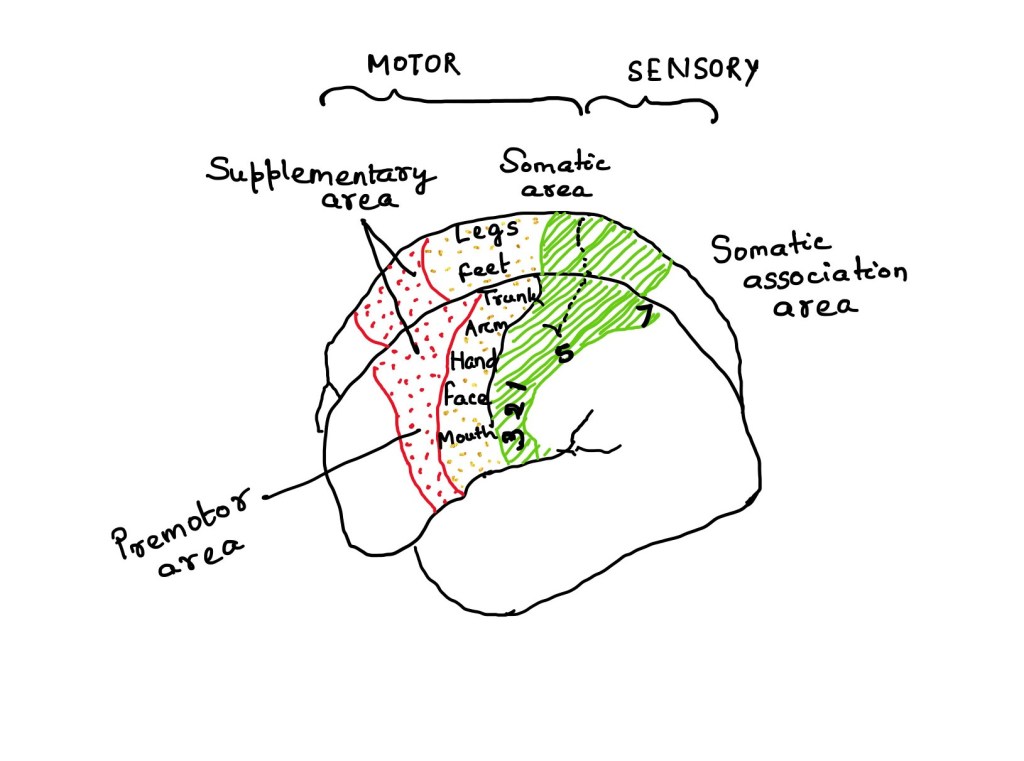
SUPPLEMENTARY MOTOR AREA
- Medial portion of Area 6 (Anterior & Medial to M1, largely on medial surface of hemisphere)
- High electrical stimulation–> Head & Eye movement, vocalization & complex postural movement.
- Somatotopic arrangement like M1 —Face, Anterior. Legs, Posterior.
- Bilaterally connected through Corpus callosum
- Subdivided into 2 areas

- FUNCTION :
- Planning & integration of complex (fixations)attitudinal movements.
- more active in bi-manual tasks
- learning of skilled acts.
- LESION –> Transient speech deficit (Aphasia) — typically disappears after several weeks. Slowness in generating repetitive movement. Retards the movement of opposite limb.
PRE-MOTOR AREA (PMC)
- High stimulation – Proximal musculature
- minor contribution to Cortico-spinal Tract.
- Major contribution to Extrapyramidal Tracts.
- FUNCTIONS:
- Responsible for patterning & posturing
- LESION:
- Weakness of opposite shoulder/ hip muscle
- limb movement slower
- Inability in simultaneous coordinated movement of both limbs
- 2 Subdivisions : DORSAL & VENTRAL
CINGULATE MOTOR AREA (CMA) within Cingulate Sulcus
CMA- r –> Rostral
CMA – d –> Dorsal
CMA – v –> Ventral
3 CMA, each with somatotopic map, contribute to CST. High stimulation similar to motor cortex stimulation.
- FUNCTION :Preparation & execution of movement.
OTHER IMPORTANT AREAS
- FRONTAL EYE FIELD — Controls eye movement
- POSTERIOR PARIETAL CORTEX — (5,7)
- Lesion : No motor weakness, but sensory & motor neglect in opposite hemifield —> AMORPHOSYNTHESIS
- BROCA’S AREA — Motor speech area, Area 44.
- Lesion : Motor aphasia
- SUPPRESSOR AREAS (4s, 2s, 8s, 19s, 24s) — Inhibition of strech reflex

HISTOLOGICAL STRUCTURE OF MOTOR CORTEX
3 Types of cells are present – 1. PYRAMIDAL CELLS 2.STELLATE/GRANULE CELL 3. FUSIFORM CELLS
6 layers or laminae are present–>
- most afferent fibers from the specific nuclei of thalamus make synapses in the laminae I to VI
- Afferent projections from non-specific thalamic nuclei & from ascendind reticular system terminate in al laminae of cortex
- Laminae II & IV are concerned with sensorial modalities.
- Laminae III to V are meant for somatomotor or visceromotor activities.
- Laminae I to VI are engaged for integration of association of sensorimotor behaviour.

