Concepts are the keystones in the architecture of our thinking.
-Paul Hughes
Let’s create road-maps for concepts.
WISDOM IS NOT A PRODUCT OF SCHOOLING BUT OF THE LIFELONG ATTEMPT TO ACQUIRE IT. –Albert Einstein
Hey there!
Let’s just say that studying can be fun too. Preparing concept map has been my thing always. So, now I am here to share my view and maps on physiology/medical topics with the world out there.
A Physiology Professor by profession I have seen students struggling with the basic concepts of the subject and almost everyone scrambling for notes (self-made, borrowed from seniors or copied from a fellow classmate). But I have found that more than so called ‘notes’, you need a clear concept – hence the concept maps.
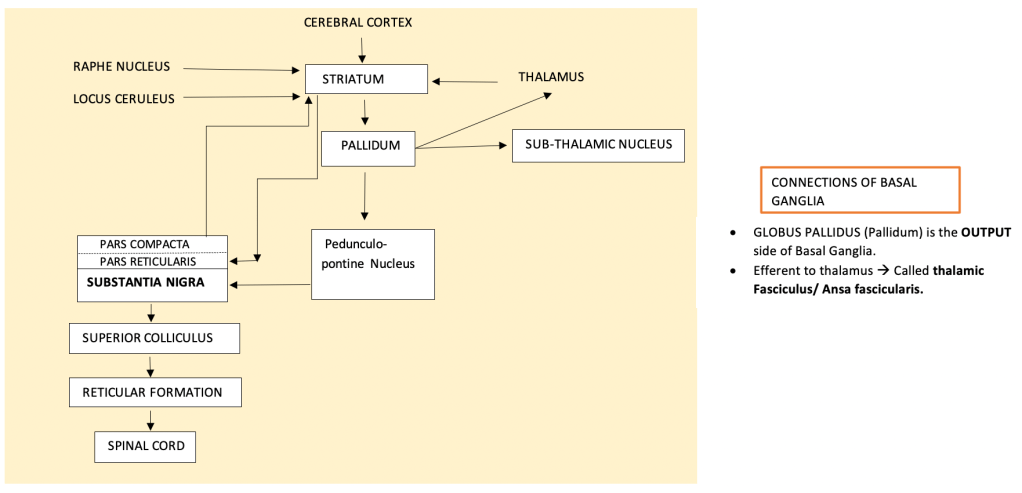
WHAT IS A CONCEPT MAP?
It is basically a conceptual diagram that suggests or compiles a knowledge or information in form of a arrow diagram or a flow chart. In other words it explains and organizes a complex information in an easy to comprehend diagram or chart. A very useful and organized way to understand, acquire & memorize concepts.
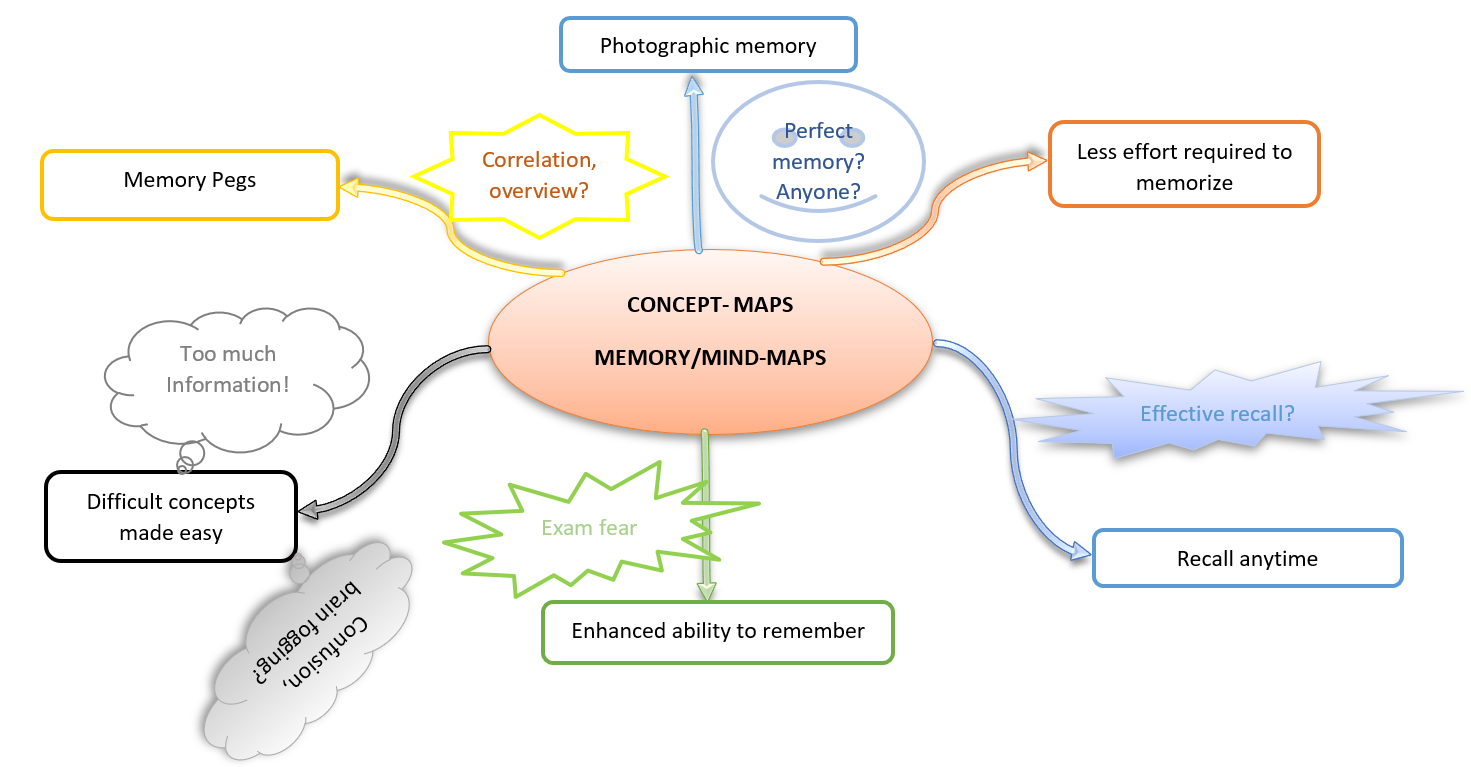
ADVANTAGES OF CONCEPT MAPS –
- Simplifies understanding of an complex phenomenon/ subject.
- helps in quicker learning. You can finish a bigger chapter in lesser time.
- easy to remember and reproduce in exams.
- creates memory maps(with less confusions of course!!)
So, see you all later in my subsequent posts where I will share my ‘concept-maps’ mostly related to Physiology, medicine & maybe everything else in due course of time. keep me posted on your view on the same.